

CAPS’ Outsourced Compounding Service
 The Lawnwood Regional Medical Center & Heart Institute is a 341-bed community hospital, a provisional level II trauma unit, and a primary stroke center. Our facility provides a broad array of services ranging from open-heart surgery to obstetrics and includes a level II neonatal intensive care unit.
The Lawnwood Regional Medical Center & Heart Institute is a 341-bed community hospital, a provisional level II trauma unit, and a primary stroke center. Our facility provides a broad array of services ranging from open-heart surgery to obstetrics and includes a level II neonatal intensive care unit.
In 2008 Lawnwood had 44,000 emergency room visits and 15,449 inpatient admissions with our pharmacy-based Nutrition Support Service providing clinical support and monitoring for 2,470 patient-days of adult total parenteral nutrition (TPN) administration. Our facility provides protein-carbohydrate (2 in 1) TPN as a 24-hour supply-per-day with lipids administered by a separate infusion. In April 2009, we opened a new trauma center, thereby signaling an increased workload to these already high numbers.
Facing Increased Demands
With the opening of the new trauma center, we saw not only an increase in overall patient volume, but also an increased level of patient acuity. Due to the resultant demands for pharmacy services, we began investigating outsourcing our TPN compounding to Central Admixture Pharmacy Services (CAPS). We compared the cost of the outsourced service to the cost of our in-house process of compounding TPN, including the FTE hours of our pharmacists and technicians who worked on compounding. At baseline, our pharmacy worked with an automated compounding machine for macronutrient base solutions, with additive syringes prepared manually by technicians. Pharmacists are required to check macronutrients on the compounder, approve each base solution, and check the additive syringes. The cost of the compounder was rolled into the daily cost for the tubing set. The compounder’s software provided an inventory utilization report each day detailing the quantity of base solutions required and specified the final TPN bag volumes. Historical usage data indicated that 85% of the daily TPN solutions were
1,000-1,999 mL, 10% were 2,000-2,999 mL, and 5% were 3,000 mL or larger.
Material and Hard Cost Comparison
In running our analysis, we developed a spreadsheet to track material and time expenses during 30 consecutive days in late September and early October of 2008. The macronutrient quantity was rounded up to the nearest base solution bag size (2,000 mL) required to complete the daily compounding, allowing for the unused solutions wasted each day to be factored into the calculation. We calculated the base solution costs plus the cost of TPN tubing divided by the number of bags made that day. We added an additional $6 to the total for syringes, needles, and the empty IV bag. The costs of the additives were not included as these costs were generally negligible. Lipid costs were not included either, as they would be unchanged. Using this information, we calculated the average cost per patient, per day. On average we were compounding nine TPN per day (range, six to13) and the cost per patient-day ranged from a low of $36.35 to a high of $44.66 for materials only. The variation in cost was largely due to amino acid solution waste.
The cost of receiving compounded TPNs from CAPS is determined by volume in liters. Knowing our cost per day and daily volume averages allowed us to make a valid comparison. While the material cost of TPN compounding plus delivery charge ended up being practically cost neutral, outsourcing would allow for additional cost and time savings in the form of redirected pharmacist services.
Refocusing Pharmacist Services
Over the 30-day trial period, pharmacists spent an average of 180 minutes per day (20 minutes per TPN per day) participating in TPN compounding and quality assurance. Our technicians also averaged 180 minutes per day in TPN compounding, restocking, and ordering of supplies. By eliminating these time-consuming tasks, we were able to redirect pharmacist time to issues of regulatory compliance. In particular, we focused on The Joint Commission’s (TJC) National Patient Safety Goal for monitoring anticoagulation services. Prior to using CAPS, our pharmacists managed all therapeutic heparin and direct thrombin inhibitor dosing within the hospital for a total of 4,500 patient-days each year. This service left little time to follow warfarin dosing. We completed a pilot study of warfarin monitoring and determined the need for 10 additional minutes to review each patient daily when no intervention was required. Based on 7,531 warfarin doses per year in 2008, 200 minutes each day were needed to meet TJC’s requirements. Prior to CAPS, we only had 60 minutes per day for warfarin monitoring, allowing for review of only 50% of daily warfarin doses, with less than 20 interventions per month for missing INRs or doses.
Implementation Results
Following the implementation of CAPS, our pharmacists were able to monitor warfarin daily from 2:00 pm to 5:00 pm, instead of having to monitor TPN compounding. During the first two months of the new program, our pharmacists were able to monitor 100% of all warfarin days. They documented 160 INR results that were ordered but not obtained, and 47 daily doses of warfarin that had not been ordered. These missing INRs and dose interventions took place prior to 5:00 pm daily allowing the nurses to obtain labs and communicate with the physicians during office hours rather than after the offices closed.
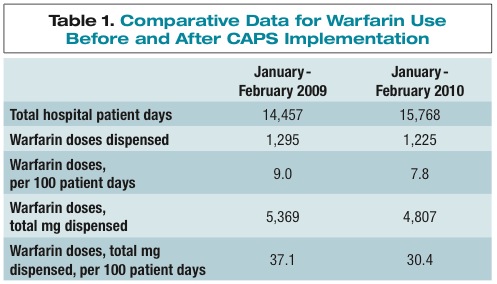
Data from January and February of 2009 were compared to the same months in 2010 after CAPS implementation. We tracked warfarin doses and total hospital patient-days in order to control for changing hospital volume. Our results (see Table 1) indicate that the warfarin dosing process was more efficient as the hospital used less doses of warfarin adjusted for patient volume. We intend to retrospectively review these data to determine if the warfarin monitoring was associated with a shorter length of stay.
While we have plenty of data demonstrating the positive impact outsourcing our TPNs has had on operations, the satisfaction gained as a result of this process change is incalculable. Mark Newnham, PharmD, BCPS, BCNSP, is the clinical coordinator at Lawnwood Regional Medical Center & Heart Institute in Fort Pierce, Florida. Mark is also a clinical instructor of Pharmacy Practice for NOVA Southeastern University in Fort Lauderdale, Florida, and Palm Beach Atlantic University in West Palm Beach, Florida.
Mark Newnham, PharmD, BCPS, BCNSP, is the clinical coordinator at Lawnwood Regional Medical Center & Heart Institute in Fort Pierce, Florida. Mark is also a clinical instructor of Pharmacy Practice for NOVA Southeastern University in Fort Lauderdale, Florida, and Palm Beach Atlantic University in West Palm Beach, Florida.
Like what you've read? Please log in or create a free account to enjoy more of what www.pppmag.com has to offer.
Recent Popular Articles






Current Issue
