

Enhance Outpatient Pharmacy Services With Centralized Fulfillment

Currently, Eskenazi Health pharmacies are operating at or near capacity with limited room for service expansion, and a challenging labor market further constrains capacity. Improving efficiency and automating commodity-type prescription filling work offers an opportunity to better leverage the pharmacy workforce for high-value work.
Eskenazi Health provides more than one million outpatient visits each year to the residents of the greater Indianapolis, Indiana community. Eight health-system retail pharmacies are co-located within community health center clinics. Rapid growth in pharmaceutical spending due to increased utilization and price inflation, coupled with a challenging reimbursement landscape, necessitates a comprehensive margin management strategy for pharmacies. With these considerations in mind, the Eskenazi Health pharmacy department crafted a multi-year strategic plan to establish a high-value pharmacy enterprise.1
Establishing a centralized pharmacy call center and distribution facility is a key component of the larger ambulatory pharmacy strategic plan. Centralizing specialty pharmacy operations offers a strategy to effectively manage high-cost specialty pharmacy inventory to prevent waste, optimize the pharmacy revenue cycle, and navigate operational complexities. To remain relevant, pharmacies must adapt to shifting consumer expectations around convenience and access.
Centralize Pharmacy Fulfillment
A centralized pharmacy fulfillment center (CFC) that incorporates significant automation supports increases in prescription filling efficiency and capacity, allowing for service expansion. Additionally, a CFC positions the pharmacy department to re-envision the ambulatory care pharmacy model to achieve patient care and population health goals in a value-based care delivery model.
Pharmacy leadership pitched the CFC concept to the health system executive leadership, who then approved a formal business review and plan development. A consultant with CFC experience was engaged to assist with this work, a process that can take 3 to 6 months. A final business plan was approved by health system leadership and the project moved to implementation. The Eskenazi Health Pharmacy CFC is divided into two spaces: a production facility for outpatient pharmacy prescription fulfillment, and a call center for customer service and patient care coordination activities. The services planned for the CFC and some of the key benefits are outlined in TABLE 1.

There is no standard industry definition for a pharmacy fulfillment center; the spectrum of services, from mail-order prescription processing to centralized sterile compounding, varies widely among facilities based on organizational needs. While no two fulfillment centers are the same, a project of this scope requires meticulous planning to evaluate the financial viability, automation options, and operational workflows. By sharing the lessons learned throughout this planning process, we hope to aid other facilities interested in establishing a CFC.
Financial Analysis
Estimating the financial and operational impact of centralizing refill services is crucial for justifying the investment in a new facility, services, and equipment. The pro forma for the CFC considers steady annual volume growth, the limitations of current pharmacies, and the potential for offering new services. Our analysis compares the projected growth over 5 years with and without a centralized service center equipped with advanced automation. Our team, with the assistance of experienced consultants, invested significant time and effort into creating a reliable pro forma to support the funding request. The pro forma included key components to highlight the impact of centralized services and service expansion:
- Prescription volumes
- Revenue
- Staffing expenses
- Operating expenses
- Operating income (ie, net profit)
- Capital recovery (ie, payback period for initial investment)
The pro forma projected that the increased filling capacity and additional volume generated, coupled with minimized staffing costs through automation, would enable recovery of the initial investment by the fourth year, versus maintaining the status quo.
Centralizing pharmacy prescription services offers a multitude of opportunities beyond those captured in a pro forma. It paves the way for new career trajectories for employees, especially in technology related roles, as they engage in the development and implementation of innovative systems and processes. Additionally, it enhances patient satisfaction through efficient delivery and outreach services, ensuring timely access to medications and personalized care. Moreover, centralization enables pharmacists to expand their roles beyond traditional dispensing, freeing up more time for patient facing services like medication therapy management, vaccinations, and collaborative practice. This shift can enrich the pharmacist-patient relationship while contributing to improved health outcomes and increased revenue potential for the pharmacy.
Identify Key Stakeholders
The collaboration of stakeholders is critical for the successful development of a CFC. Leveraging the expertise of various roles is essential in the planning and design of a CFC. Outside of the pharmacy department stakeholders may include representatives from the business development and strategy, project management, facilities management, and security teams. These stakeholders met weekly during the CFC design process to develop the comprehensive business plan. In addition, various groups held separate meetings throughout the design process to address critical tasks within their scope. With a solid plan in place, we proceeded to automation selection and facility development.
Centralize Specialty Pharmacy
Offering specialty pharmacy services was another key driver in our decision to pursue a central fill model. Eskenazi Health did not have an accredited specialty pharmacy and retrofitting an existing location to meet accreditation standards was not feasible. Specialty pharmacies necessitate a robust and distinct care delivery model compared to traditional community pharmacies. In addition, these services require a specialized team that is adept in insurance benefits investigations, prior authorizations, clinical monitoring, delivery coordination, and refill management.
Coordinating these services is already intricate and the specialty pharmacy market is only going to increase in complexity. With new cell and gene therapies becoming available, combined with the likelihood that dozens of gene therapies will be developed through 2030, there needs to be intentional coordination and robust operations provided by the specialty pharmacy team.2 Centralizing the resources required for specialty pharmacy services within a CFC can offer a structural intervention to promote standardization of practice and enhance communication within the specialty team.
In establishing a CFC for specialty pharmacy services, facilities can help align accreditation requirements with robust operational improvements. The demand for pursuing CFC pharmacy services in tandem with specialty pharmacy services continues to expand. Implementing a CFC can help consolidate medication and packaging supplies, mitigate staffing hours, automate filling processes, and support call center capabilities for CFC pharmacy services. In one study, implementation of a CFC resulted in an almost 50% reduction in the time pharmacy team members spent on CFC prescription filling and packaging tasks.3 This study also found a decreased call abandonment rate as well as reductions in pharmacy workload resulting from an overall reduction in call center volume as the rate of first-call issue resolution increased. As health systems expand and innovate to service the complex specialty market demands, tracking specialty pharmacy metrics may offer helpful data points for making the case to build a CFC (see TABLE 2).

Operational Workflow
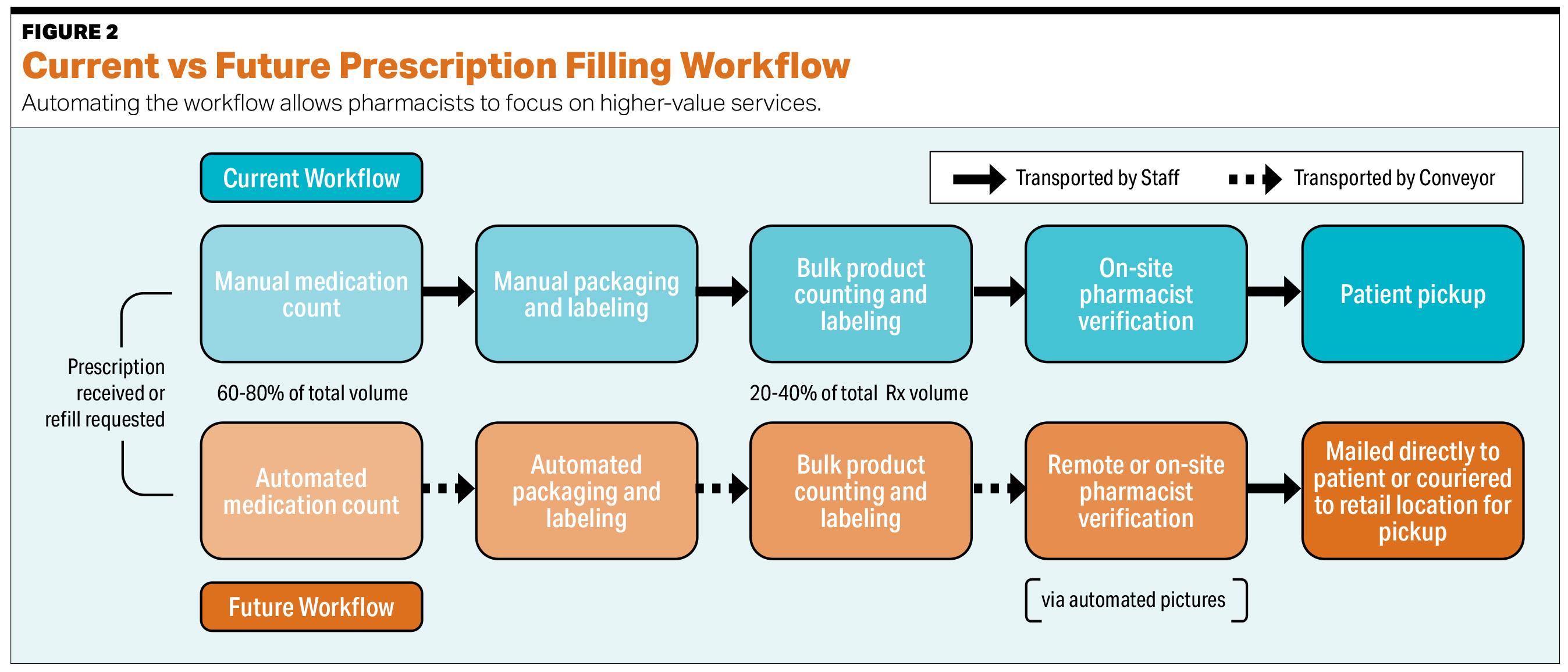
The priority for the operational workflow at the CFC centers on using automation to reduce the redundancies in our existing outpatient pharmacy processes. Currently, most prescriptions are filled with minimal automation, limited mainly to dated pill counters for processing high volume medications, while staff directly manage dispensing, labeling, and packaging. Additionally, medications are manually transported through the various stages from fill stations to verification and dispensing. Implementing cutting edge filling technology and conveyor-based automation significantly reduces the manual labor required for these tasks (see FIGURE 1). See FIGURE 2 for a comparison of current versus future packaging workflows.

Click here to view a larger version of this FIGURE.
Click here to view a larger version of this FIGURE.
With the new system, a large portion of outpatient prescriptions will be processed using a conveyor belt setup. First, robotic machines will handle the filling of high volume oral solids. The next station will manage unit-of-use products requiring label application, followed by the manual counting of low volume oral solids. Successive steps will manage processing of specialty medications, refrigerated items, and controlled substances. Completed orders will be verified by a pharmacist and sent to packaging and shipping for direction to the ultimate destination, be that delivery to the pharmacy or directly to the patient.
Currently, our facility uses 60 FTEs to dispense over 900,000 prescriptions per year. Any increase in prescription volumes has historically required staff growth. However, based on our pro forma estimates, we anticipate that prescription volumes will increase by nearly 30% over the next 5 years, while staffing needs will rise by only about 7%. These efficiency gains will allow us to dedicate resources to support expanded services, such as medication delivery and the implementation of expanded ambulatory services.
Automation Vendor Selection
When selecting an automation vendor for an outpatient pharmacy CFC, thorough research and evaluation are crucial. Initiate the process by requesting proposals (RFPs) from multiple vendors to compare their offerings and pricing. It is essential to request demos and visit existing installations. Speaking directly with current customers can offer invaluable insights into the vendor’s customer service, and the solution’s effectiveness in real-world settings.
Tour facilities with similar volumes, service scopes, and EHRs early in the evaluation process. These visits provide crucial knowledge and feedback regarding the implementation process and ongoing product support. Furthermore, use these visits to establish connections with staff who can share their experiences of working in a pharmacy fulfillment center, including the impact on personnel and any aspects they would alter if given the chance to restart the implementation process.
Take care to assess the scalability and flexibility of the automation systems to ensure alignment with your facility’s current requirements and future growth projections. Consider factors such as integration capabilities with existing pharmacy management systems and adherence to regulatory compliance standards. Additionally, prioritize vendors with a proven track record of innovation and commitment to ongoing support to stay ahead in the constantly evolving landscape of healthcare.
Determine Facility Location
After finalizing the services to be offered and identifying the necessary automation, the next step is finding a suitable facility. We employed space planning techniques to determine the necessary areas for drug storage, automation infrastructure, supply storage, compounding, delivery services, compliance packaging, and essential amenities like offices, breakrooms, and restrooms. It is imperative to envision future needs, given the substantial investment involved and our intent to occupy the site for at least 10 years. This approach ensures we do not model the workflow to meet current requirements alone, in an effort to avoid future regrets.
After determining the required square footage, we selected a suitable location based on factors such as real estate values, proximity to our target areas, and convenient access via well-connected roads. We intentionally chose a site near the interstate loop encircling Indianapolis, ensuring swift and effective access to all serviced locations.
Conclusion
Centralized services provide significant opportunities to increase efficiency, expand offerings, and improve patient service in the outpatient pharmacy space. Our strategic decision to explore a retail pharmacy fulfillment center was driven by an evaluation of current challenges, a changing pharmacy environment, and the availability of technology and operational solutions. As the practice of pharmacy evolves beyond simply dispensing medications, proactively anticipating and preparing for future growth is the key to optimizing pharmacy services.
References
- Rough S, Shane R, Armitstead JA, et al. The high-value pharmacy enterprise framework: Advancing Pharmacy Practice in health systems through a consensus-based, strategic approach. Am J Health Syst Pharm. 2021;78(6):498-510. doi:10.1093/ajhp/zxaa431
- Young C, Quinn C, Trusheim C. Durable cell and gene therapy potential patient and financial impact: US projections of product approvals, patients treated, and product revenues. Drug Discovery Today. 2022;27(1):17-30. doi:10.1016/j.drudis.2021.09.001
- Kappenman A, Ragsdale R, Rim M, Tyler LS, Nickman NA. Implementation of a centralized mail-order pharmacy service. Am J Health Syst Pharm. 2019;76: S74-78.

Christopher Wickesberg, PharmD, MBA, BCPS, is the director of pharmacy at Eskenazi Health pharmacy enterprise. In his more than 20 years with the organization, Christopher helped guide the move to a new facility, implement a new EHR, and is leading pharmacy practice model advancement. He received his PharmD from Purdue University.

Todd B. Cox, PharmD, is a manager for the outpatient pharmacies at Eskenazi Health in Indianapolis, Indiana. He received his PharmD from Purdue University. In Todd’s 22 years as outpatient pharmacy manager, he has overseen the construction or remodeling of seven pharmacies.

Katelyn Gordon, PharmD, MHA, BCPS is the pharmacy manager for specialty pharmacy services at Eskenazi Health. She is responsible for coordinating the formalization of specialty pharmacy services and leading accreditation efforts. Prior to this role, she attended pharmacy school at Butler University and completed a PGY1/PGY2 health system pharmacy administration and leadership residency training at the University of Iowa Hospitals and Clinics.

Kala L. Sanders, PharmD, MBA is the pharmacy operations manager at Atrium Health Cabarrus in Concord, North Carolina. She attended pharmacy school at Butler University and completed residency training at Eskenazi Health in Indianapolis, Indiana. Kala was employed at Eskenazi Health from 2018 to 2024 in roles which included clinical pharmacy technician, medication access specialist II, and PGY1/PGY2 health system pharmacy administration and leadership resident.

Samuel P. Lewis, PharmD, MS, 340B ACE, is the pharmacy business manager at Eskenazi Health. He received his PharmD from Purdue University and MS in health system pharmacy administration from The Ohio State. In Sam’s over 5 years with the organization, he has overseen 340B program compliance, medication procurement, and pharmacy revenue integrity.
Like what you've read? Please log in or create a free account to enjoy more of what www.pppmag.com has to offer.
Recent Popular Articles






Current Issue
